
I was originally going to write this post for the 4th of July, given the subject matter. However, as regular readers know, I am not unlike Dug the Dog in the movie Up, with new topics that float past me in my social media and blog reading rounds serving as the squirrel. Then I got a copy of the movie VAXXED to review last week, and before I knew it this post had been delayed two weeks. Never let it be said, though, that I don’t circle back to topics that interest med. (Wait, strike that. Sometimes, that actually does happen. It just didn’t happen this time.) This time around, I will be using documents forwarded to me by a reader as a means of revisiting a discussion that dates back to the early days of this blog. (Or is it the other way around?)
The return of the revenge of “battlefield acupuncture”
Today’s topic is the Veterans Health Administration (VHA) and its embrace of pseudoscience. VA Medical Centers (VAMCs) provide care for over 8 million veterans, ranging from the dwindling number of World War II and Korean War veterans to soldiers coming home now from our wars in Iraq and Afghanistan. Although there have been problems over the years with VAMCs and the quality of care they provide, including a recent scandal over hiding veterans’ inability to get timely doctors appointments at VAMCs, a concerted effort to improve that quality of care over the last couple of decades has yielded fruit so that today the quality of care in VA facilities compares favorably to the private sector. Unfortunately, like the private sector, the VA is also embracing alternative medicine in the form of “complementary and alternative medicine” (CAM), or, as its proponents like to call it these days, “integrative medicine,” in order to put a happy label on the “integration” of pseudoscience and quackery with conventional medicine.
Of course, I (and others at SBM) have discussed the intrusion of woo into the military before. For instance, a post I wrote in SBM’s first year of existence discussed Col. (Dr.) Richard Niemtzow, a radiation oncologist by training but also one of the Department of Defense doctors trained as certified acupuncturists, and his advocacy for “battlefield acupuncture.” The form of acupuncture that Col. Niemtzow advocated was auricular acupuncture, which involves inserting tiny needles into the ear and leaving them there until they fall out. He even pioneered a program to train physicians in “battlefield acupuncture” and deploying them to combat zones. Not surprisingly, the evidence base cited in support of such a program was—how do I put this?—underwhelming, but that hasn’t dampened enthusiasm for the idea and other alternative medicine in the military. Given that my last post on battlefield acupuncture was in 2009, I thought I’d take a look again at the infiltration of “integrative medicine,” including battlefield acupuncture, into the military and the VHA. Unfortunately, unlike Clay Jones’ satirical—or…is it?—piece about robotic acupuncture, this is no joke. It’s really happening.
Not surprisingly, where the military goes, it doesn’t usually take too long for the VHA to follow, largely because its patient base is veterans and many of its physicians come from military medicine backgrounds. Indeed, there is even an organization called the Defense and Veterans Center for Integrative Pain Management (DVCIPM), which has teamed with the Department of Defense (DoD) and the VHA to set up a program called Acupuncture Training Across Clinical Settings (ATACS), to promote battlefield acupuncture (BFA):
ATACS will be deploying certified Battlefield Acupuncture (BFA) trainers to receptive Department of Defense/Veterans Affairs (DoD/VA) medical centers to teach this technique to qualified providers and collect data to assess patient and project outcomes. The intent is that these trained providers will act as “sustainers” and assist with the ongoing incorporation of Acupuncture into practice within the MHS/VHA. Under the discretion of the DoD/VA medical facility leadership, ideal candidates would be physicians, nurses, any healthcare provider that has pain management responsibilities either at the Medical Treatment Facility (MTF) or deployed.
Yes, you read that right. The intent of this program is to “integrate” acupuncture into routine practice in the VHA and DoD medical facilities. Even now, the VHA is claiming:
The Battlefield Acupuncture technique is a unique auricular (ear) Acupuncture procedure developed in 2001 by then Air Force Colonel Richard Niemtzow, M.D, to train Physicians, Physician Assistants, Nurse Practitioners, and other providers to treat pain throughout the MHS and VHA. This technique provides a much needed alternative in cases where the initiation or continuation of opioid analgesics is deemed clinically risky, in cases where current medications and other therapies are not working, and cases where the existence of and potential for substance abuse, addiction and tolerance issues make medication therapies impractical.
The BFA course – usually 1-2 half days – teaches non-acupuncturist clinical providers the BFA technique. Training in BFA offers providers the opportunity to enhance their clinical practice skills in musculoskeletal and pain management conditions by adding Battlefield Acupuncture technique to their “tool bag.” It is hoped that this technique will be a primary or secondary modality to reduce the use of opioids and habit forming drugs.
If acupuncture is, as David Colqhoun and Steve Novella so aptly put it, nothing more than a theatrical placebo, then auricular acupuncture is placebo without a lot of the theatrics. What impressed me most about the FAQ on BFA published by the DVCIPM (see, I can use alphabet soup acroynyms and abbreviations like the ones the military uses too) was the utter lack of scientifically compelling evidence. All there is, except for an ancient (2002!) functional MRI study is a small unblinded pilot study that I’ve discussed before, larger unblinded study using a grab bag of different forms of acupuncture, discussed here, and study of the “feasibility of introducing BFA into the aeromedical evacuation system.”
Typical of CAM research, this is putting the cart before the horse. First, it should be established that a treatment actually works (i.e., is efficacious and safe). Only then should studies examining the feasibility of integrating the treatment into the aeromedical evacuation of wounded soldiers be undertaken. Unfortunately, this is a metaphor for what the VHA is doing: integrating unscientific and unproven CAM modalities in the absence of compelling evidence to treat, in particular, chronic pain and post-traumatic stress disorder (PTSD), both unfortunately very common afflictions of veterans, particularly combat veterans.
Yet, the VHA is charging full steam ahead to “integrate” dubious treatments into its array of offerings.
Lots of CAM in the VA, we need more, more more…
One of the documents a reader sent me was the report, FY2015 VHA Complementary and Integrative Health (CIH) Services (formerly CAM). I note that “complementary and integrative health” (CIH) seems to be the new government-sanctioned term for CAM, as reflected not only in this report but in the recent renaming of the National Center for Complementary and Alternative Medicine (NCCAM) to the National Center for Complementary and Integrative Health (NCCIH). One could view this as just another step in the evolution of “integrative medicine.” Be that as it may, this report is very revealing, particularly taken in context of the history of CAM/CIH use in the VHA, as represented by major “achievements” touted by the VHA, not the least of which is a 2011 VA survey showing that 9 out of 10 VHA facilities offer at least some CAM/CIH and the expansion of VA funding for studying CAM treatments for PTSD in the same year, because there was “scant evidence” from randomized controlled clinical trials. This report is more recent; so let’s take a look.
Here are some of the key findings of the FY2015 report:
- Most administrative parent facilities offer at least one CIH service to Veterans (93% in 2015 vs. 89%in 2011).
- Although many facilities offer CIH services, the availability of these services is limited. In facilitiesoffering an individual CIH service, only acupuncture, chiropractic, mindfulness, Stress Management Relaxation Therapy (SMRT), acupressure, and movement practices are offered at a rate equivalent toat least one half day per week.
- CIH services are offered in all the VA clinical care settings inquired about in this survey.
- Most CIH services are offered by VA providers, however, a portion of this care is provided by WithoutCompensation (WOC) providers. The most common CIH services being provided by WOC providersinclude Yoga (58%), Animal Assisted therapy (52%), and Tai-chi/Qi gong (36%).
- Chiropractic care and acupuncture are the two modalities most likely to be referred to non-VA careproviders by a VA facility.
- Of the 131 sites offering CIH services, the top perceived factors enabling services are that CIH is consistent with patient-centered model of care (122 sites), promotes well-being (121 sites), beingadjunctive to chronic disease management (109 sites), as well as patient preference (104 sites).(Table 1.b.)
- Providers’ perception of the top three services for which veterans are asking for more offerings include acupuncture (80%), chiropractic (80%), and massage therapy (81%).
Here are the sorts of CIH/CAM offered at VHA facilities (click to embiggen):
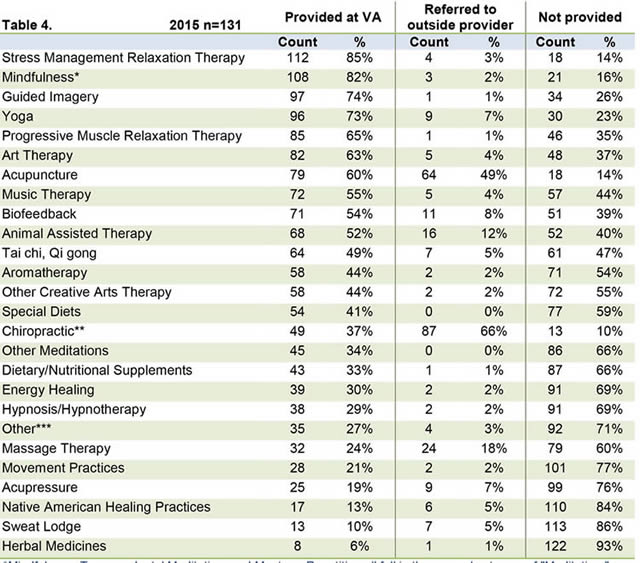
One notes a lot of the usual modalities rebranded as somehow being “CAM/CIH,” such as diet, exercise, relaxation, and the like, but there are also acupuncture, which is a modality based on the vitalistic principles of traditional Chinese medicine (TCM), such as the flow of qi, or “life energy.” There’s also chiropractic, and, as I like to say, chiropractors are incompetent physical therapists with delusions of grandeur, which tells me all the funds wasted on chiropractic would be better used hiring more physical therapists at VHA facilities. And what is this with 13% of VHA facilities offering sweat lodges and 30% offering “energy medicine,” which encompasses reiki, therapeutic touch, and other forms of what can only be described as pure quackery?
The naturopaths pounce
As I like to point out any time the topic comes up, naturopathy is a hodge podge of modalities ranging from traditional Chinese medicine, to reflexology, to supplements, to applied kinesiology, to just about any pseudoscientific medicine you can think of, all mixed with a dollop of diet and lifestyle co-opted from science-based medicine to give the quackery a patina of seeming scientific respectability. All you really need to know to know how bad naturopathy is this: The One Quackery To Rule Them All, homeopathy is an integral part of naturopathy, takes up many hours of instruction in naturopathy schools, and is featured on the NPLEX, the naturopathic licensing examination. In other words, you can’t have naturopathy without homeopathy.
Predictably, last fall, seeing the open embrace with which the VHA is inviting quackery into its VAMCs, naturopaths saw their opening and decided to pounce on this opportunity. The largest “professional” organization for the quacks known as naturopaths, the American Association of Naturopathic Physicians (AANP, which unfortunately shares an abbreviation with the American Association of Nurse Practitioners and must be distinguished from such a respectable organization) has teamed up with American Veterans (AMVETS) to lobby Congress to pass a bill that would pay for “natural, non-pharmacological approaches to treating veterans suffering from chronic pain“:
AMVETS, one of the nation’s largest veterans service organizations, has joined with the American Association of Naturopathic Physicians (AANP) in seeking to promote natural, non-pharmacological approaches to treating veterans suffering from chronic pain.
The organizations have collaborated via a “Dear Colleague” letter in the US House of Representatives calling on the Department of Veterans Affairs (VA) to take steps to employ licensed naturopathic physicians, who are specially trained in natural, non-invasive methods of healing. A “Dear Colleague” letter to that effect has begun circulating in the US House of Representatives. Leading the charge is Congressman Mark Pocan (D-WI), who – like many of his colleagues – is concerned about the dangers of overmedicating veterans, especially with painkilling opioids. Rep. Pocan is joined by Representatives Julia Brownley (D-CA), Suzan DelBene (D-WA), Earl Blumenauer (D-OR), Raul Grijalva (D-AZ), and Walter Jones as the letter’s initial signators.
“After incidents across the country of veterans overdosing on or abusing opioids associated with chronic pain, it is clear we need a new approach to veterans’ pain management,” Rep. Pocan stated. “Our veterans deserve access to all possible forms of care when making their healthcare decisions, including the services provided by naturopathic doctors (NDs).”
So let’s see. Rep. Pocan’s argument, fed to him no doubt by the AANP and facilitated by AMVETS, seemed to boil down to this: Opiate pain relievers, as effective as they are, have a downside, including dependence, addiction, and overdosing. If anything, since last September, this argument has become more potent, given the recent news coverage of the high level of opioid dependence and death in the US. Because of these problems, a common problem with opioids is that physicians are often overly cautious prescribing opioids, resulting in undertreatment of chronic pain. What “non-pharmacologic” treatments of chronic pain would help? Neither the AMVETS press release nor Rep. Pocan’s “Dear Colleague” letter said.
More importantly, how would our veterans be provided access to naturopathic care? AMVETS, the AANP, and Rep. Pocan urged VA Secretary Robert McDonald to assign an employment code to licensed NDs so that they can be brought into the agency’s healthcare system. Right now, apparently, NDs (or, as I like to refer to them, “not a doctor”) cannot be on staff at VA hospitals and VA facilities right now, which is good. There is no employment code for them.
How would our veterans be provided access to naturopathic care? AMVETS, the AANP, and Rep. Pocan urge VA Secretary Robert McDonald to assign an employment code to licensed NDs so that they can be brought into the agency’s healthcare system. Right now, apparently, NDs (or, as I like to refer to them, “not a doctor”) couldn’t be on staff at VA hospitals and VA facilities right now, which is good. There was no employment code for them.
But why? Why should the VA change its policy and allow NDs to be on staff at VA facilities in order to offer naturopathic modalities to our veterans? The AMVET press release trotted out the usual misinformation and naturopathy talking points:
For military veterans, chronic pain often coexists with other health problems such as posttraumatic stress disorder (PTSD), depression, anxiety, and sleep disturbances. NDs are well suited to help, since they are specially trained in natural, non-pharmacological approaches that facilitate the body’s self-healing ability.
Approximately 4,400 NDs are licensed to practice naturopathic medicine, having earned their degree from 4-year postgraduate naturopathic medical schools accredited through the US Department of Education. The approaches studied include nutritional counseling and stress reduction, botanical medicine, therapeutic manipulation, and oriental medicine. A strong emphasis is placed on disease prevention and educating patients on proactive self-care to maintain wellness. Resolutions passed by the US Senate have urged Americans to learn more about this “safe, effective, and affordable form of health care.”
No. As has been described by “naturopathic apostate” Britt Hermes, naturopathic education is nowhere near the equivalent of the education conventional physicians receive in medical school and their clinical residencies and fellowships. Naturopathic research is rife with unethical practices, and the accreditation of naturopathic education is a sham. None of this stopped Tracy Gaudet, MD, director of the VHA’s Office of Patient Centered Care and Cultural Transformation from, while speaking at last fall’s annual DC Federal Legislative Initiative held by the American Association of Naturopathic Physicians, characterizing naturopathy as “a huge answer for the country, for practice, for patients” that is available “at a pivotal transformational moment” in health care and referring to them as “pioneers” who have been practicing integrative medicine “all along.” One notes that, before being hired by the VHA, Dr. Gaudet was a very high profile promoter of “integrative medicine,” having served as the director of Duke Integrative Medicine, a “pioneer” institution in quackademic medicine, as well as, before that, the founding director of the University of Arizona Program in Integrative Medicine with Dr. Andrew Weil.
The plan: Advancing Complementary and Integrative Health in VHA
I revisited “battlefield acupuncture” intentionally at the beginning of this post, using it as an introduction to survey the breadth and depth of “integrative medicine” offered at VAMCs, because it is a glaring example of how deeply quackery has embedded itself into military medicine and the VHA. It thus didn’t surprise me (although it depressed me) to be sent this memo from the Co-Chairs of the Veterans Experience Committee (VEC) to the Under Secretary for health, dated May 3, 2016 under the subject of “Advancing Complementary and Integrative Health in VHA.” The memo is disturbing for a number of reasons, which is why I provide a link to the PDF, for readers who wish to read the whole thing themselves. Because it’s a scanned document that’s 11 pages long, I won’t be typing everything, but I will cite key points in selected excerpts.
First:
VA is shifting the current culture of health care from problem-based “sick care” to “whole health care,” which engages and inspires Veterans to their highest level of health and well-being. The Office of Patient Centered care and Cultural Tranformation (OPCC&CT) and the Veterans Experience Committee (VEC) have worked with VHA leaders and clinical champions across the system to work towards this transformative goal. One aspect of this mission includes the promotion of complementary and integrative health (CIH) services such as acupuncture, mind-body techniques, yoga, and massage, within the VA healthcare system. CIH services promote self-healing and complement conventional (or allopathic) medical approaches to support Veterans on their path to health and well-being. In 2013, VHA established the Integrative Health Coordinating Center (IHCC) within OPCC&CT. The IHCC is charged with developing and implementing CIH strategies in clinical activities, education, and research across the system. Its two major functions are: (1) to identify and remove barriers to providing CIH across the VHA system; and (2) to serve as a resource for the clinical practices and education for both Veterans and clinicians. Thus, the IHCC supports VHA’s strategic plan and the MyVA plan to provide Veterans with “Access to Innovative Health Care.” Implementation of CIH services across the enterprise directly supports VA’s Strategic Goal #1, to “empower Veterans to improve their well-being,” and the VHA Strategic Goal #1, “provide Veterans personalized, proactive, patient-driven health care.” This is reinforced by the sustained high degree of congressional interest and support for CIH services, including sections 441 and 442 of the proposed bill S.425. The IHCC receives weekly inquiries of the types and and availability of CIH services within the VA.
I was unfamiliar with S.425; so I looked it up. It’s the Homeless Veterans’ Reintegration Programs Reauthorization Act of 2015. It’s a bill to reauthorize homeless reintegration programs in the VA until 2020, which is an odd place to put anything about CAM. Be that as it may, this memo makes it very clear that it is official VHA policy not only to offer CAM or CIH services, but to actively promote it and remove barriers to providing CIH services across the entire VHA system, which in military-government jargon means forcing providers to offer them, much as advocates have tried to force residents to learn and offer CAM/CIH. Indeed, the above paragraph is chock full of government bureaucratic jargon combined what Kimball Atwood used to call the “Weasel Words of Woo,” complete with rhetoric about moving from “sick care” to “whole health care”; “patient-centered” or “patient-driven” care, which is frequently co-opted to justify the integration of quackery; empowering patients (in this case, Veterans with a capital V); and, of course, “personalized” care. (My head was hurting by the end of this, so thick was the government jargon mixed with “weasel words of woo.”)
The purpose of the memo is to request “review and approval” of the Under Secretary of Health a “recommended path forward to provide policy, guidance, and regulatory change required to implement CIH services that meet the definition of basic care as described in the standard Medical Benefits Package (38 CFR 17.38(b)).” The VEC notes that “high priority” areas for the “integration” of CIH services in the VHA include chronic pain management, mental health conditions (e.g., anxiety, depression, and PTSD), and chronic disease management (e.g., cardiovascular disease, hypertension, diabetes, and obesity). Also, according to the VEC, the vetting process for new CIH modalities will include:
- Clinical evidence
- Licensing and credentialing
- Clinical practice guidelines, current evidence, community standards, and potential for harm
- Veteran demand, although it is noted that “the clinical need and appropriateness of any treatment is based on the clinical judgment of the provider and services are not provided solely at the request or preference of the patient” (imagine my relief).
- Supports transformation of healthcare delivery (whatever that means)
As far as “clinical evidence, the VEC cites the Institute of Medicine recommendation that the same “principles and standards” of evidence should appl to all treatments, but then it immediately starts special pleading for CIH, noting that the “characteristics of some CAM therapies—such as variable practitioner approaches, customized treatments “bundles” (combinations) of treatments, and hard-to-measure outcomes—are difficult to incorporate into treatment-effectiveness studies,” which is true. It’s also true that these “characteristics are not unique to CAM” but are “more frequently found in CAM than in conventional therapies.” What is more common in CAM is special pleading that these difficulties should be excuses for accepting a lower standard of evidence. If, for instance, I were to make the sorts of pleas that I hear from CAM practitioners about, for example, genomic-based personalized, or precision, medicine, where difficulties in randomization and doing clinical trials are epic (a topic I might review again in the future), CAM advocates would lambaste me for special pleading—and rightly so. What I fear is what happens so often with CAM: That a lot of pseudoscience will be “integrated” into VHA offerings based on dubious evidence. It’s already happened with auricular acupuncture, after all.
Also I fear this, straight from the memo:
Adjustments to VHA business processes will be required to provide infrastructure of CIH service delivery across VHA. Additionally, CIH services may need to compete for resources with existing VHA programs. These processes have begun and will be reinforced by the clarification provide by this memo.
Yes, barring increased appropriations from Congress (highly unlikely), every dollar directed to CIH services in the VHA is a dollar redirected from science- and evidence-based treatments currently offered. It is a zero-sum game, and the VEC knows that. Even so, Under Secretary David Shulkin approved the memo.
Indeed the process had already begun long before this memo was sent to the Under Secretary, and is continuing. It is, unfortunately, a very big deal because the VHA runs the largest healthcare system in the US and has a great deal of influence because of that. Just as the VA pioneered the use of electronic medical records in the 1990s, it could be now “pioneering” the infiltration of quackery into an enormous health care system.
Our veterans deserve much better than this. They deserve the best science-based medicine we can offer. Unfortunately, thanks to “competition for resources” by an ever-growing CIH program at the VA and “marching orders” demanding more CIH/CAM, they are likely to be getting more woo and less science-based medicine.
from Science-Based Medicine http://ift.tt/2a9BN8C
No comments:
Post a Comment